2016 NEJM--Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit
Purpose:
The best timing for RRT in ICU patients with AKI is unknown.
Despite progress in RRT management, mortality remains high and the timing of its initiation remains open to debate when no metabolic disorder (severe hyperkalemia or metabolic acidosis) or major fluid overload threaten short term prognosis. Such abnormalities mandate RRT and are non-inclusion criteria of our study.
=> whether duration of oliguria/anuria and /or value of serum urea/creatinine are an adequate indications for RRT is unknown.
Hypothesis:
“Delayed” strategy would prove beneficial to the patients and would translate into increased survival.
=> This study is designed to prove superiority (and not noninferiority) of this strategy over the “early” one.
Objective:
Main objective to compare two strategies of RRT initiation in terms of overall survival in ICU patients (mechanically ventilated and/or receiving catecholamine infusion) with severe AKI defined as RIFLE F classification.
Early strategy
|
Delayed strategy
|
RRT immediately when a RIFLE F status is documented
|
RRT in patient with RIFLE F only in case of occurrence of one or more of the follow events (“Alert Criteria”):
|
Design: Prospective, multicenter, randomized, open-label trial comparing two RRT initiation strategies in terms of overall survival
Primary endpoint:
Overall survival, measured from the date of randomization to the date of death, regardless of the cause. Minimun duration: 60-day follow-up
Secondary endopoints:
- survival rate at D28
- % of patients requireing who did not require RRT in the delayed strategy
- timie unitl cessation of RRT therapy
- Rate of adverse events potentially related to the AKI or to RRT (eg; RRT catheter related complicates, hemorrhage due to anticoagulation required for RRT etc…)
- rate of nosocomial infections
- # of vetilator free days of RRT free days and of vasopressors free days
- length of stay in ICU and hospital
- rate of limitations of treatment for futiligy
- total cost of connsumables (including RRT catheters and lines among others) related to RRT between D1 and D28
Inclusion criteria:
- ICU patients
- Age > = 18 years
- AKI compatible with the dx of ATN defined by clinical ischemic or toxi insult
- AKI, with RIFLE F classification: (one of the following 3)
- Creatinine > 354 mmol/L (4mg/dL) or > 3 times the baseline
- anuria for more than 12 hours
- oliguria defined as U/O < 0.3ml/kg/hr or 500ml/d for more than 24 hours
- Mechanical ventilation and/or catecholamines infusion (noradrenaline or/and adrenaline)
Non-inclusion criteria:
- CKD (defined as creatinine clearance < 30ml/min)
- Patients already enrolled in the study
- Inclusion criteria #4 present for more than 5 hours
- AKI due to
- urinary tract obstruction
- renal vessels obstruciton
- tumor lysis syndrome
- thrombotic microangiopathy
- acute GN
- Intoxication with a dialyzable product
- Child-Pugh class C liver cirrhosis
- Renal transplant
- Cardiac arrest without awakening at time of potential inclusion
- Moribund state
- decision to limit treatment
- RRT already started for the current episode of AK
- Presenting (at time of potential inclusion) a strong indication for immediate RRT
- oligoanuria for more than 3 days
- Alert criteria
- Under cardiopulmonary bypass
- Included in another clinical trial on RRT modalities

Result:
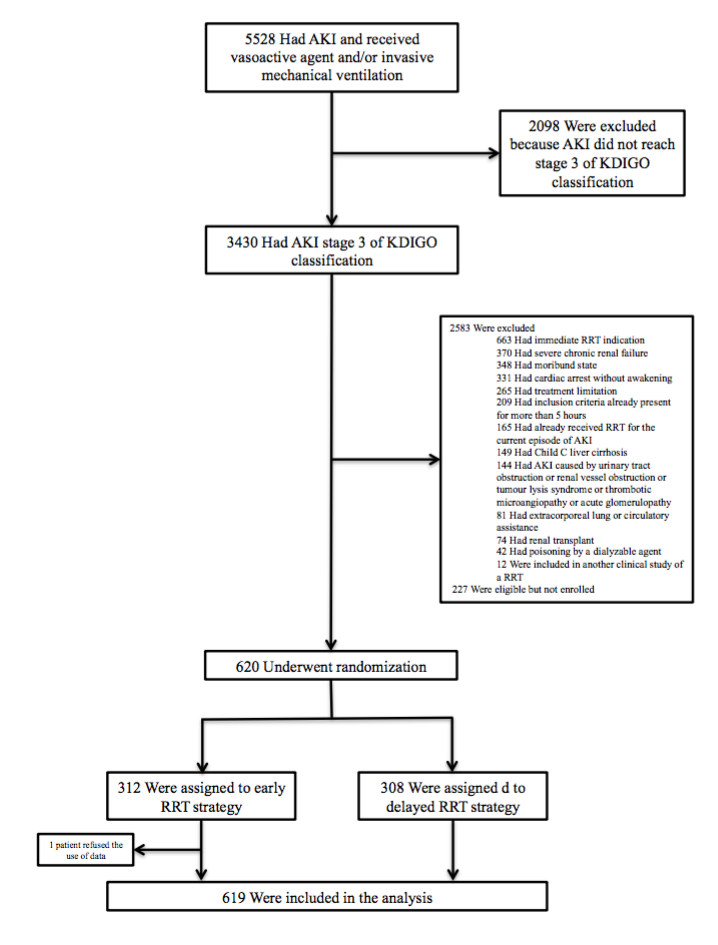
- early group:
- Late group: 157 receiving RRT ⇔ 101 w/o RRT, and the number in the late group with RRT are below:

- The patients’ condition at the timing of RRT initiation:
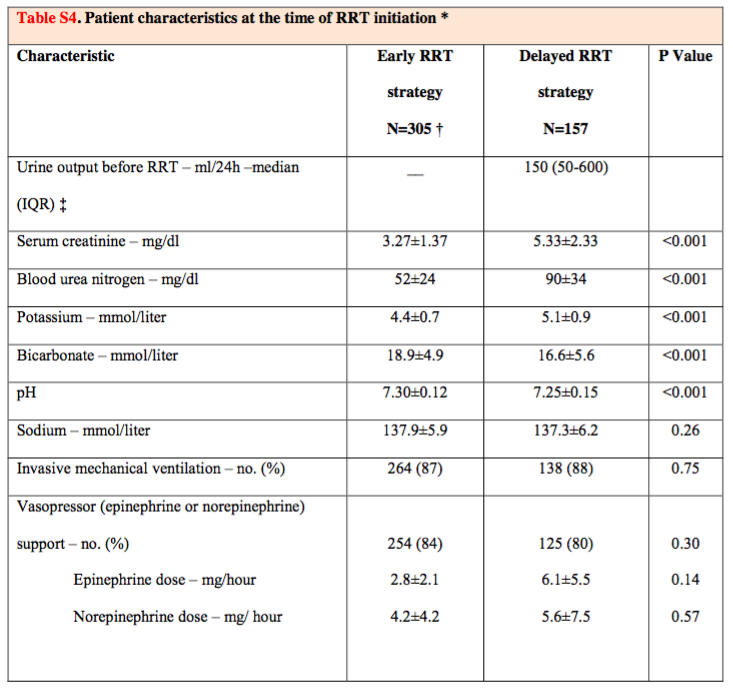
Metabolic abnormalities were more marked in the delayed strategy group than in the early strategy
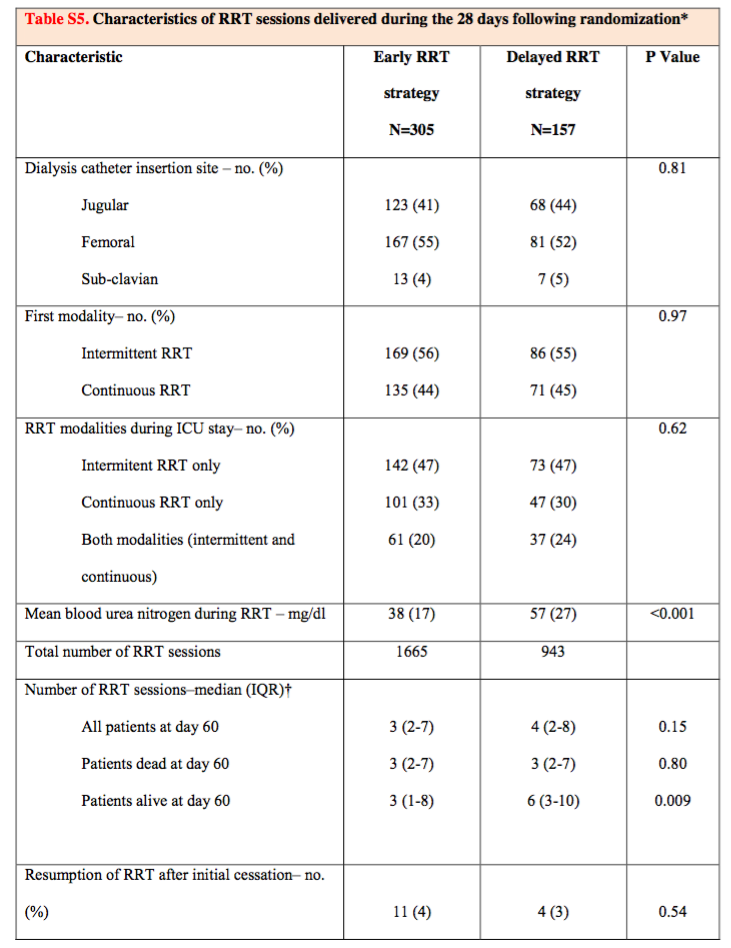
- Whether there is different modality or condition between the two group?
Early group
|
Late
| |
deaths at day 60
|
150
|
153
|
mortality at Kaplan-Meier
|
48.5%
|
49.7%
|
overall mortality at D60
|
49.1%
| |
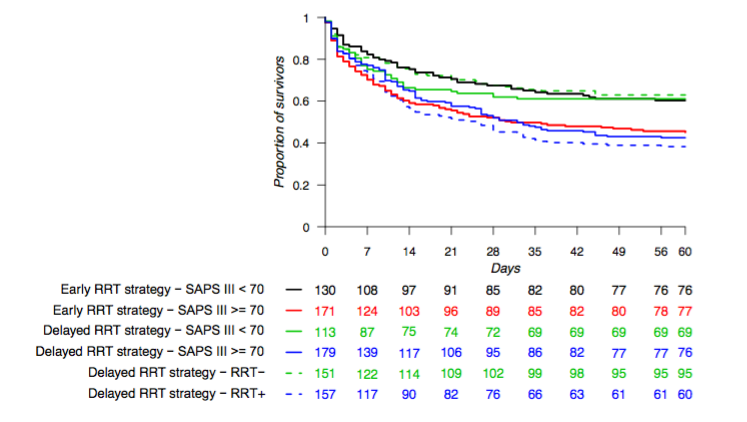
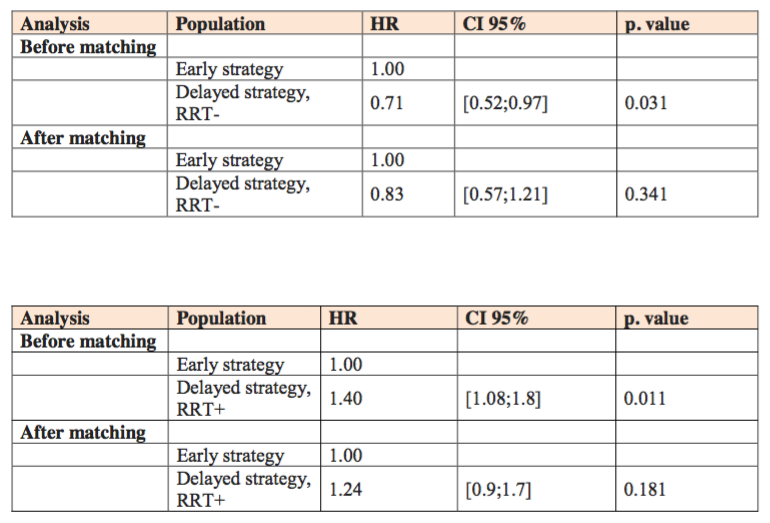
- Post hoc exploratory analysis
Early
|
Late - RRT
|
Late + RRT
| |
D60 Mortality
|
48.5%
|
37.1%
|
61.8%
|
Baseline severity SOFA (Med)
|
11
|
10
|
12
|
Adjustment for severity
|
non-significant
  | ||
The # of days free from RRT
|
lower (17)
|
higher (19)
| |
CRBSI
|
higher (10%)
|
lower (5%)
| |
Hypophosphatemia
|
higher (22%)
|
lower (25%)
| |
Hemorrhage of other etiologies
(other than GIB or dialysis catheter)
|
lower (0.3%)
|
higher (4%)
| |
Adequate diuresis w/o RRT
|
Earlier
| ||
 | |||
Discussion
- No survival benefit was observed with the delayed strategy of RRT
- The recovery of renal function, as marked by diuresis, was more rapid and catheter relted infections occurred less frequently in the delyaed-strategy group than in the early-strategy group
- Lengths of stay in the ICU and in the hospital were similar in the two groups
- Allowing time for renal funciton recovery did not lead to prolongation of the stay in the ICU
- This study is not generalizale => > 50% iHD first + only 30% CRRT alone
Limitations:
- The power of the study to distriguish a significant difference in mortality could be questioned
- Not using Kt/V to evaluate the dose of RRT => However, the study keep serum urea low during therapy
- The study group is “advanced” AKI => may not be generalizable to patients with different KDIGO stages of AKI
- 有些人可能會把這個研究在接受Late-strategy這組的高致死率詮譯作一個”late strategy”有害的效果 (deleterious effect)。然而,在接受到”late RRT"的這組病人(比起不是接受”late RRT”的那一組)明顯有比較差的疾病狀況;並且進一步地對疾病嚴重程度加以校正來看的話,會發現所觀察到的crude difference是受到干擾的(was confounded)。
" Our study should not be interpreted as suggesting that a “”wait and see” approach is safe for all patients.” => Careful surveillance is mandatory when deciding to delay RRT in patients wi severe AKI….
Conclusion:
No significant difference in mortality with a strategy of delayed initiation as compared with early initiation of RRT.
沒有留言:
張貼留言