2016 CJASN--Urinary Biomarkers at the Time of AKI Diagnosis as Predictors of Progression of AKI among Patients with Acute Cardiorenal Syndrome
The primary outcome: AKI progression
The secondary outcome: AKI progression with subsequent death
Conclusions uAGT, uNGAL, and uIL-18 measured at time of AKI diagnosis improved risk stratification and identified CRS patients at highest risk of adverse outcomes.
=> Best ROC: uAGT => 0.76 in primary outcome/ 0.93 in secondary outcome
2016年10月5日 星期三
2016年7月16日 星期六

2016年6月27日 星期一



2016年6月13日 星期一
Hypothyroidism, Pseudo, Pseudo-Pseudo
Wikipedia好像整理得不錯:(應該沒錯吧?)
https://www.wikiwand.com/en/Pseudopseudohypoparathyroidism
Hypoparathyroidism
Pseudo-hypoparathyroidism
Pseudo-Pseudo-hypoparathyroidism
Pseudo-hypoparathyroidism
Pseudo-Pseudo-hypoparathyroidism

1. "假":有Imprint 的概念,GNAS1裡的一個locus
"假":有分1a, 1b, 2
2. 外觀異常只有"假1a"和"假假"
3. "假": 抽血全都異常:高雙P (PTH/Pi)+低雙C(Calcitriol/Ca)
"假假":抽血全都正常!只是長得不一樣
4. hypo-PTH: low PTH/Calcitriol/Ca,但是高Pi
5. 背genetic defect from whom: 母親or父親
"假":有分1a, 1b, 2
2. 外觀異常只有"假1a"和"假假"
3. "假": 抽血全都異常:高雙P (PTH/Pi)+低雙C(Calcitriol/Ca)
"假假":抽血全都正常!只是長得不一樣
4. hypo-PTH: low PTH/Calcitriol/Ca,但是高Pi
5. 背genetic defect from whom: 母親or父親
2016年6月7日 星期二
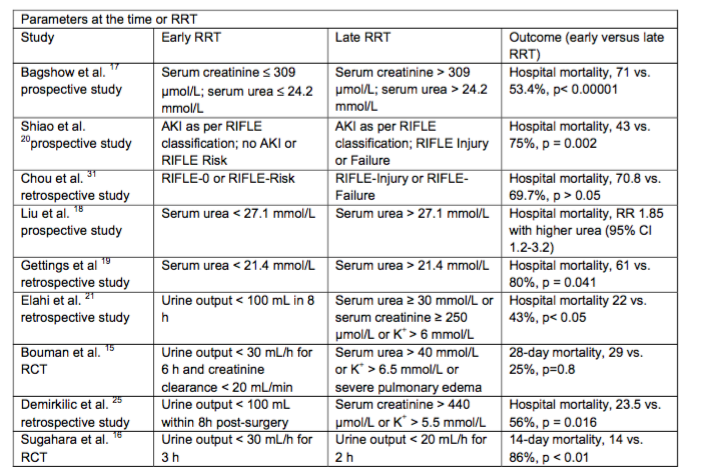
2016 RRT trial: ELAIN vs. AKIKI
From 2016 JAMA--ELAIN trial
NEJM--AKIKI (multicenter)
|
JAMA--ELAIN trial (single center)
| |
Hypothesis
|
We hypothesized that the "delayed" strategy would prove beneficial to the patients and would translate into increased survival. The study is designed to prove superiority (and not noninferiority) of this strategy over the "early" one.
|
We hypothesize that an early initiation of RRT decreases the 90-day mortality from all causes compared to late onset of RRT.
|
Study population
|
RIFLE F: early and late (or with alert criteria)
|
AKIN 2 and 3 (3 or absolute indication)
|
AKI definition
|
RIFLE F: early or late
|
AKIN stage: 2 or 3
|
Intervention
|
Arm 1: RRT immediately when a RIFLE F status is documented
Arm 2: RRT in patient with RIFLE F only in case of occurrence of one or more of the follow events (“Alert Criteria”)
|
Arm 1: Early initiation of RRT (AKIN 2)
Arm 2: Late initiation of RRT (AKIN 3 or absolute indication for RRT)
|
Primary outcome
|
Overall survival, measured from the date of randomization to the date of death, regardless of the cause. Minimun duration: 60-day follow-up
|
Overall survival in a 90-day follow up period (90-day all cause mortality)
|
Secondary outcome
|
|
|
Inclusion criteria
|
|
|
Exclusion criteria
|
|
|
Conclusions:
|
In a trial involving critically ill patients with severe acute kidney injury, we found no significant difference with regard to mortality between an early and a delayed strat- egy for the initiation of renal-replacement therapy.
A delayed strategy averted the need for renal-replacement therapy in an appreciable number of patients.
|
AmongcriticallyillpatientswithAKI,early RRT compared with delayed initiation of RRT reduced mortality over the first 90 days. Further multicenter trials of this intervention are warranted.
|
2016年6月5日 星期日
2016 AJKD--Continuous Dialysis Therapies Core Curriculum 2016--CRRT principle
2016 AJKD--Continuous Dialysis Therapies Core Curriculum 2016--CRRT principle
- Studies designed to compare continuous versus intermittent therapies have not shown a beneficial effect on mortality
- With greater hemodynamic stability and a higher likelihood of kidney recovery compared to standard iHD
- Lack of consensus on several aspects of RRT (eg, timing of initiation, dose, session lenth, and standards for monitoring.
===================================================================
- Solute transport
- convection, diffusion, and adsorption, and replenishing depleted solutes
- CVVH, relies solely on convection; CVVHD, CVVHDF, SCUF
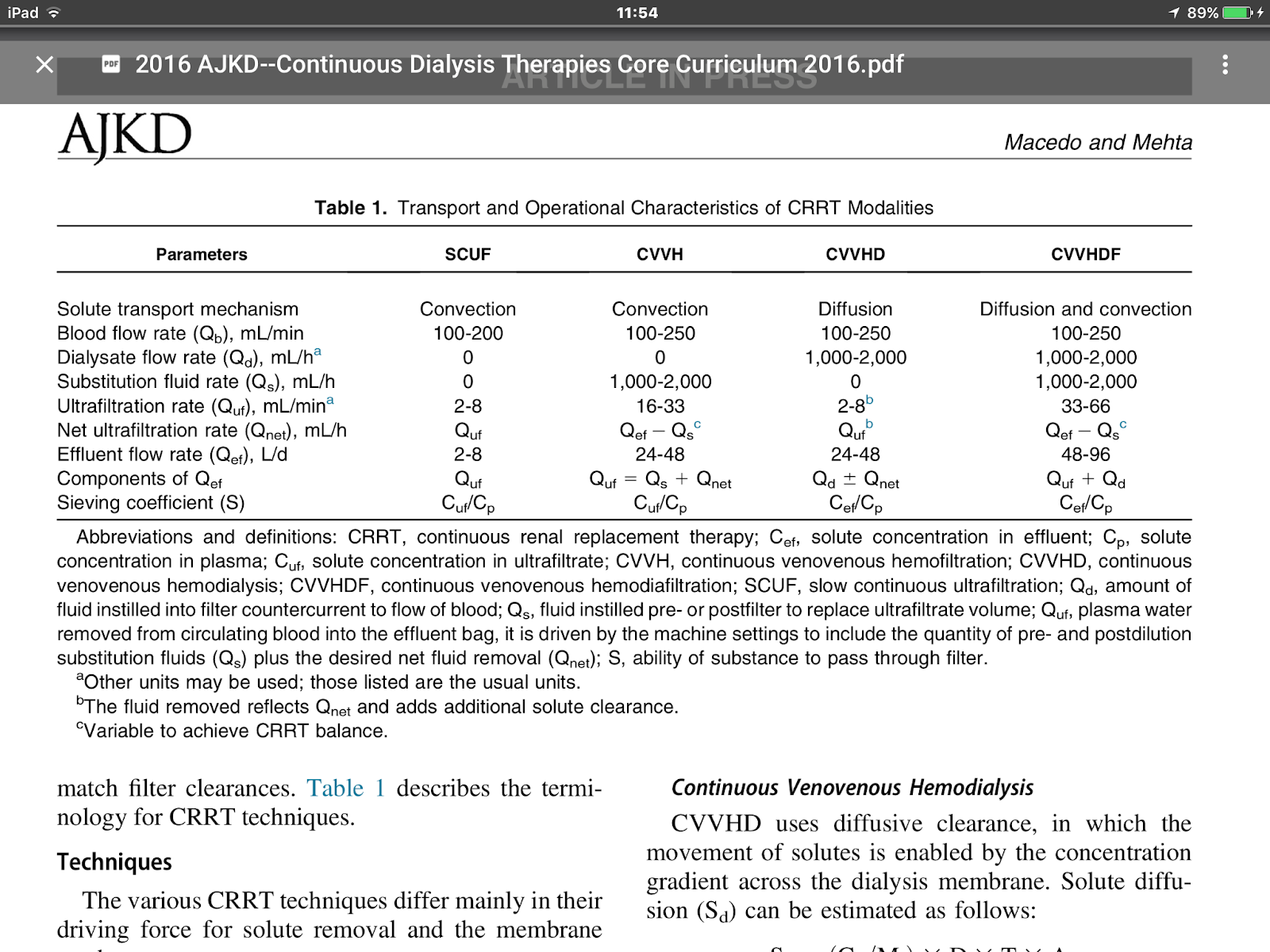
- These mechanisms can by manipulated by the type of membrane and blood and fluid flow rates to selectively influence solute clearances of moledules of different size.
Adsorption of solutes occurs to varying degrees in all CRRT circuits and can be a contributor for large molecule removal, depending on membrane characteristics.
- Effluent flow rate (Qef) is the final result of the filtration process and is composed of the net ultrafiltration (Qnet) + substitution fluid rate (Qs) in CVVH and CVVHDF + dialysate flow rate in CVVHD and CVVHDF.
=> CVVH and CVVHDF: Qef = Qnet + Qs
=> CVVHD and CVVHDF: Qef = Qnet + Qs + dialysate flow rate (????)
- Filter clearance for most CRRT = Qef * S
- S: sieving coefficient = Cuf / Cp, regulated by reflection coefficient of membranes
- reflection coefficient of memebranes => S = 1 - σ, S = 1, solute freely passes through membrane; S = 0, solute cannot freely pass through membrane
- For middle molecules: clearance depends on [membrane permeability] * UF volume
- For adsorption: overall blood clearance can be grater than filter clearance, even when S is low => blood-side clearances will not match filter clearances
- Techniques: differ in [various driving force for solute removal] and [membrane use]
- CVVH: via convection, driven by TMP:
- Uf = Kf * TMP,
- Kf = coefficient of hydraulic permeability, and
- TMP = (Pb - Puf) - 𝝿, Pb = blood hydrostatic pressure; Puf = UF/dialysate hydrostatic pressure, 𝝿 = plasma proteins oncotic pressure
- Cx = Quf * S, Cx: convection clearance, S: sieving characteristics of membane = Cuf/Cp
- Qnet = UF - substitution fluid infusion
- CVVHD: vis diffusive clearance, by solute concentration gradient acrosss the dialysis membrane
- Sd = (Cg / Mt ) * D * T * A
- Sd: solute diffusion, Cg: concentration gradient, Mt = membrane thickness, D = diffusion coefficient of the solute, T = solution temperature, A = membrane surface area
- gradient across membranes: Qd、Qb; Qd is the rate limiting factor for solute removal => Qd 0.5~3 L/h (8~50 mL/min) vs. Qb 100~200 mL/min
- CVVHDF: via diffusion + convective technique => dialysate + substitution sol.
- removal of small + middle molecules
- Slow continuous ultrafiltration (SCUF): use exclusively the principle of UF w/o substitution. => safely treat fluid overload
- solute removal is minimal because it is limited by total UF volume
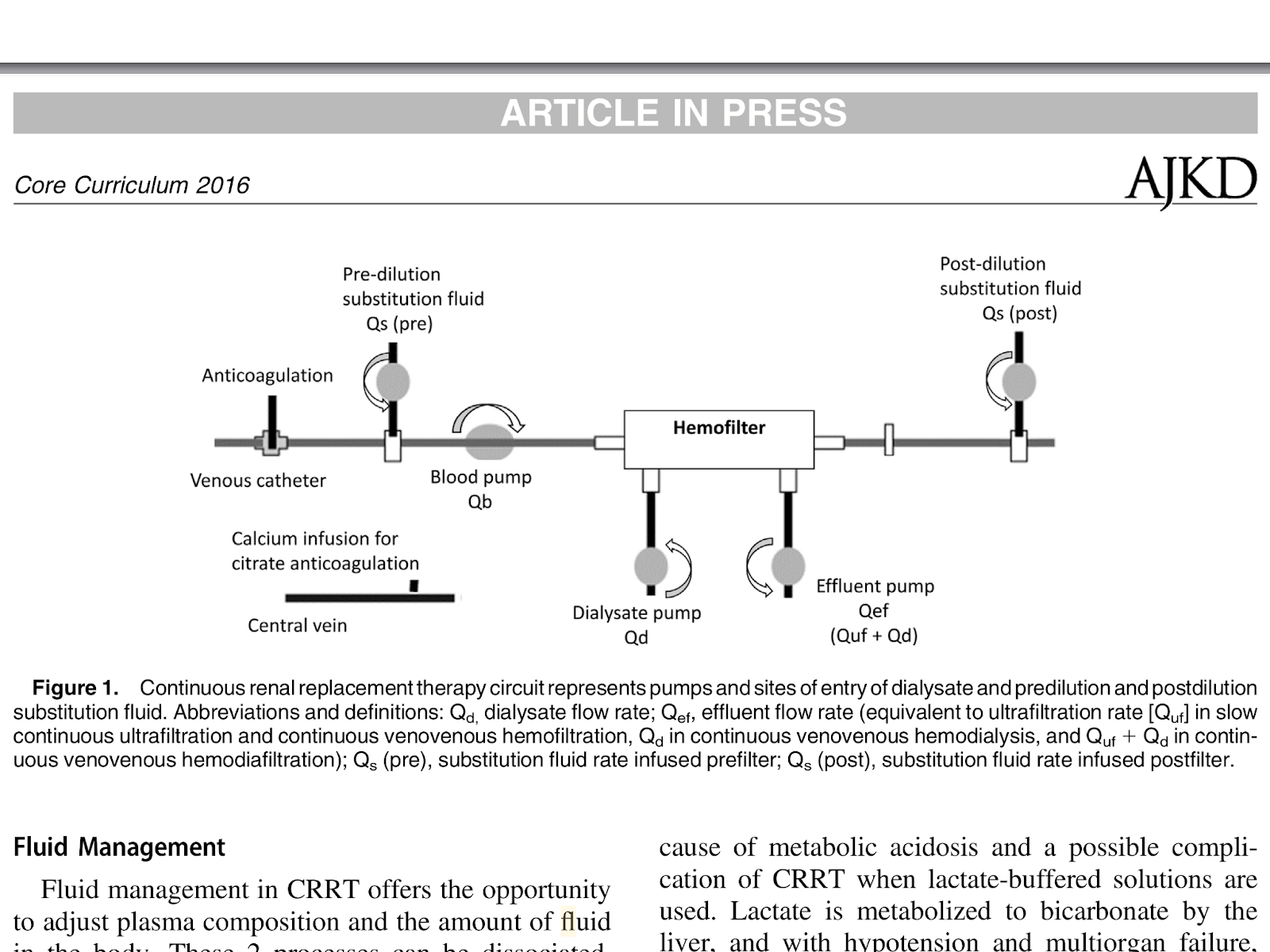
- CRRT: plasma composition + fluid amout in the body => 分開處理
Substitiuion fluid:

- Citrate is used as an anticoagulant => provides a buffer base cecause each citrate colecule is metabolized in the liver and muscle to 3 molecules of bicarbonate
=> but may leads to markedly hypotensiion
- CRRT’s key feature is the flexibility in maintaining a specific level of any electrolyte and calibrating the rate of correction to accommodate the clinical need
- The technique to achieve fluid management:
- Most common: vary Qnet to meet the anticipated fluid balance needs over 8~24 hours:
- Effluent vol + solute clearance => vary with each adjustment in net ultrafiltration
- To keep a fixed rate of UF exceeds the hourly intake from all sources and to vary the amount of post-dilution substitution fuid administered:
- ensures a constant effluent volumen and solute clearance level.
- Post-dilution fluid can be given outside the CRRT circuit through a peripheral IV line.
- Third method: fluid valance is tailored to achieve a targeted hemodynamic parameter every hour.
- such as: CVP, MAP, PAWP, etc.
2016年6月3日 星期五
2016 NEJM--Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit
2016 NEJM--Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit
Purpose:
The best timing for RRT in ICU patients with AKI is unknown.
Despite progress in RRT management, mortality remains high and the timing of its initiation remains open to debate when no metabolic disorder (severe hyperkalemia or metabolic acidosis) or major fluid overload threaten short term prognosis. Such abnormalities mandate RRT and are non-inclusion criteria of our study.
=> whether duration of oliguria/anuria and /or value of serum urea/creatinine are an adequate indications for RRT is unknown.
Hypothesis:
“Delayed” strategy would prove beneficial to the patients and would translate into increased survival.
=> This study is designed to prove superiority (and not noninferiority) of this strategy over the “early” one.
Objective:
Main objective to compare two strategies of RRT initiation in terms of overall survival in ICU patients (mechanically ventilated and/or receiving catecholamine infusion) with severe AKI defined as RIFLE F classification.
Early strategy
|
Delayed strategy
|
RRT immediately when a RIFLE F status is documented
|
RRT in patient with RIFLE F only in case of occurrence of one or more of the follow events (“Alert Criteria”):
|
Design: Prospective, multicenter, randomized, open-label trial comparing two RRT initiation strategies in terms of overall survival
Primary endpoint:
Overall survival, measured from the date of randomization to the date of death, regardless of the cause. Minimun duration: 60-day follow-up
Secondary endopoints:
- survival rate at D28
- % of patients requireing who did not require RRT in the delayed strategy
- timie unitl cessation of RRT therapy
- Rate of adverse events potentially related to the AKI or to RRT (eg; RRT catheter related complicates, hemorrhage due to anticoagulation required for RRT etc…)
- rate of nosocomial infections
- # of vetilator free days of RRT free days and of vasopressors free days
- length of stay in ICU and hospital
- rate of limitations of treatment for futiligy
- total cost of connsumables (including RRT catheters and lines among others) related to RRT between D1 and D28
Inclusion criteria:
- ICU patients
- Age > = 18 years
- AKI compatible with the dx of ATN defined by clinical ischemic or toxi insult
- AKI, with RIFLE F classification: (one of the following 3)
- Creatinine > 354 mmol/L (4mg/dL) or > 3 times the baseline
- anuria for more than 12 hours
- oliguria defined as U/O < 0.3ml/kg/hr or 500ml/d for more than 24 hours
- Mechanical ventilation and/or catecholamines infusion (noradrenaline or/and adrenaline)
Non-inclusion criteria:
- CKD (defined as creatinine clearance < 30ml/min)
- Patients already enrolled in the study
- Inclusion criteria #4 present for more than 5 hours
- AKI due to
- urinary tract obstruction
- renal vessels obstruciton
- tumor lysis syndrome
- thrombotic microangiopathy
- acute GN
- Intoxication with a dialyzable product
- Child-Pugh class C liver cirrhosis
- Renal transplant
- Cardiac arrest without awakening at time of potential inclusion
- Moribund state
- decision to limit treatment
- RRT already started for the current episode of AK
- Presenting (at time of potential inclusion) a strong indication for immediate RRT
- oligoanuria for more than 3 days
- Alert criteria
- Under cardiopulmonary bypass
- Included in another clinical trial on RRT modalities
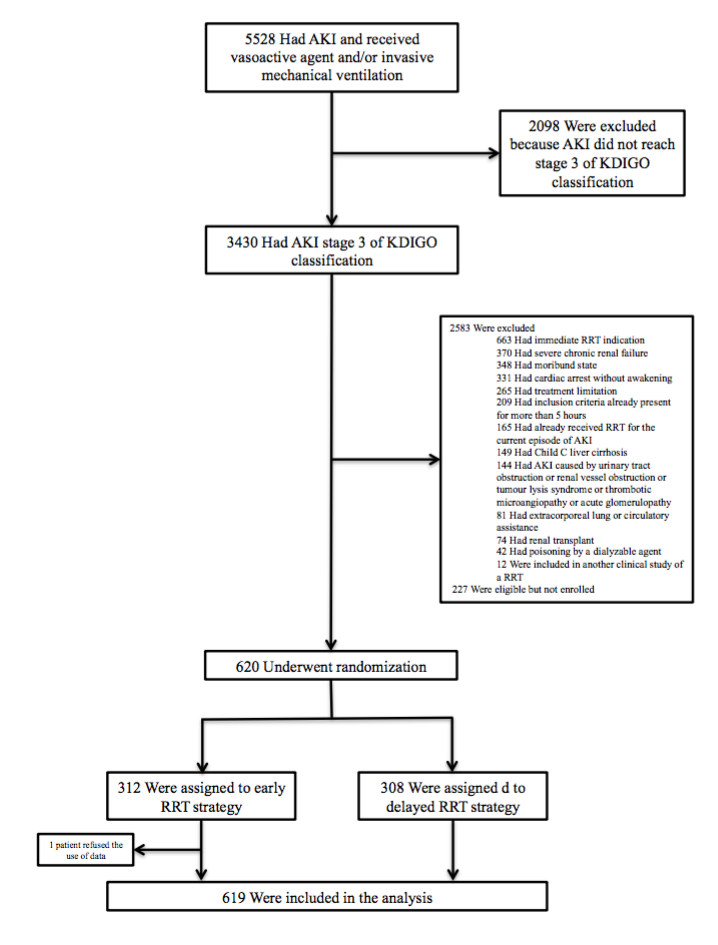

Result:
- early group:
- Late group: 157 receiving RRT ⇔ 101 w/o RRT, and the number in the late group with RRT are below:

- The patients’ condition at the timing of RRT initiation:
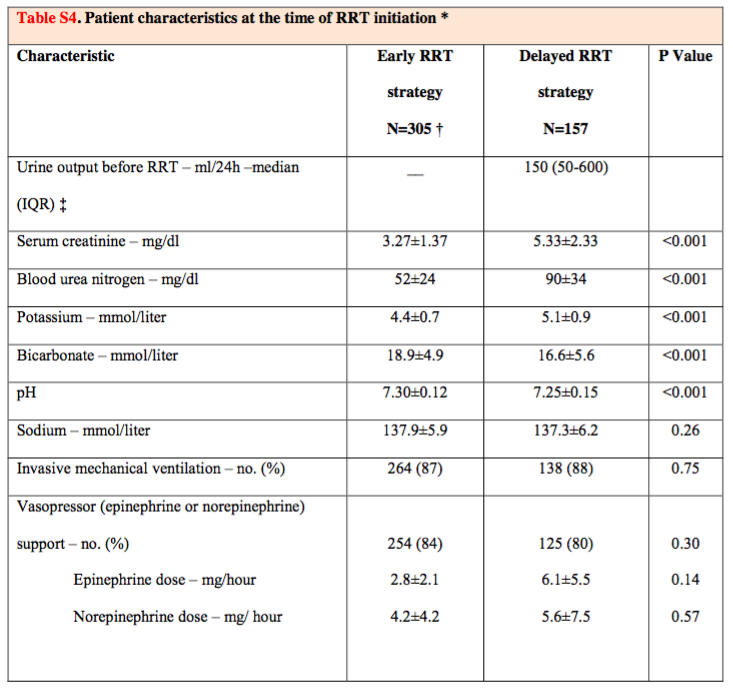
Metabolic abnormalities were more marked in the delayed strategy group than in the early strategy
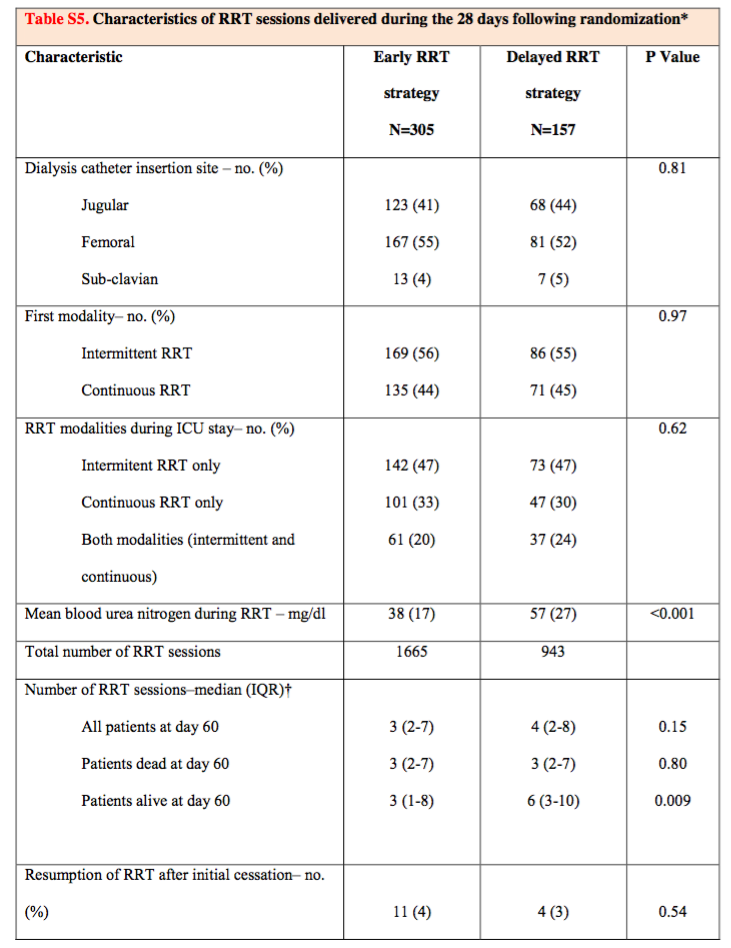
- Whether there is different modality or condition between the two group?
Early group
|
Late
| |
deaths at day 60
|
150
|
153
|
mortality at Kaplan-Meier
|
48.5%
|
49.7%
|
overall mortality at D60
|
49.1%
| |
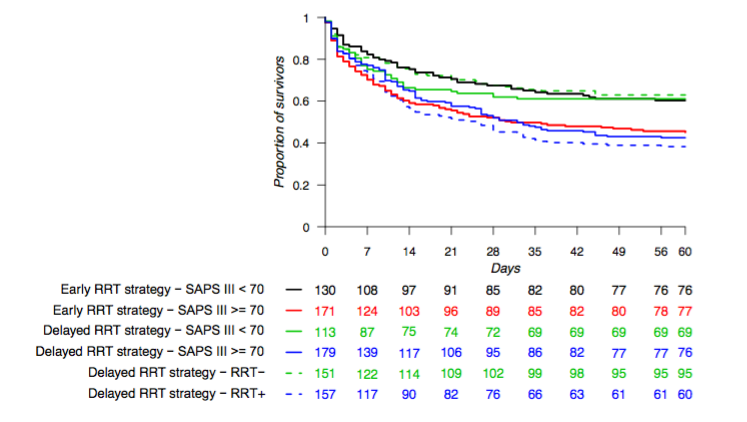
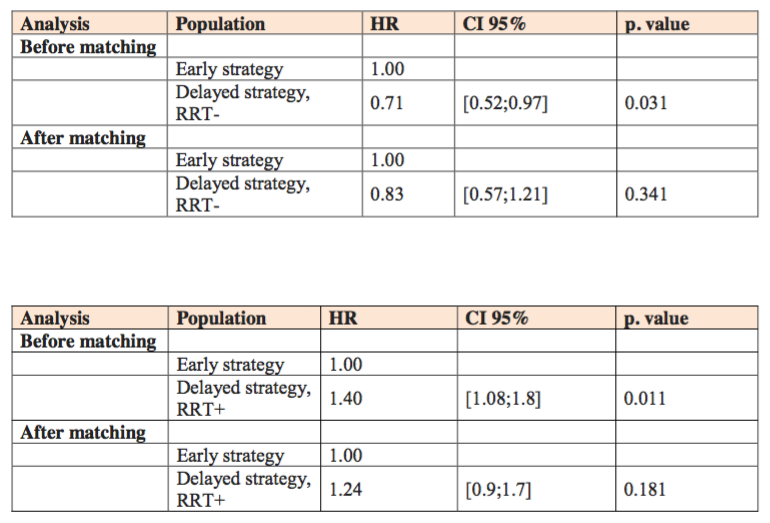
- Post hoc exploratory analysis
Early
|
Late - RRT
|
Late + RRT
| |
D60 Mortality
|
48.5%
|
37.1%
|
61.8%
|
Baseline severity SOFA (Med)
|
11
|
10
|
12
|
Adjustment for severity
|
non-significant
  | ||
The # of days free from RRT
|
lower (17)
|
higher (19)
| |
CRBSI
|
higher (10%)
|
lower (5%)
| |
Hypophosphatemia
|
higher (22%)
|
lower (25%)
| |
Hemorrhage of other etiologies
(other than GIB or dialysis catheter)
|
lower (0.3%)
|
higher (4%)
| |
Adequate diuresis w/o RRT
|
Earlier
| ||
 | |||
Discussion
- No survival benefit was observed with the delayed strategy of RRT
- The recovery of renal function, as marked by diuresis, was more rapid and catheter relted infections occurred less frequently in the delyaed-strategy group than in the early-strategy group
- Lengths of stay in the ICU and in the hospital were similar in the two groups
- Allowing time for renal funciton recovery did not lead to prolongation of the stay in the ICU
- This study is not generalizale => > 50% iHD first + only 30% CRRT alone
Limitations:
- The power of the study to distriguish a significant difference in mortality could be questioned
- Not using Kt/V to evaluate the dose of RRT => However, the study keep serum urea low during therapy
- The study group is “advanced” AKI => may not be generalizable to patients with different KDIGO stages of AKI
- 有些人可能會把這個研究在接受Late-strategy這組的高致死率詮譯作一個”late strategy”有害的效果 (deleterious effect)。然而,在接受到”late RRT"的這組病人(比起不是接受”late RRT”的那一組)明顯有比較差的疾病狀況;並且進一步地對疾病嚴重程度加以校正來看的話,會發現所觀察到的crude difference是受到干擾的(was confounded)。
" Our study should not be interpreted as suggesting that a “”wait and see” approach is safe for all patients.” => Careful surveillance is mandatory when deciding to delay RRT in patients wi severe AKI….
Conclusion:
No significant difference in mortality with a strategy of delayed initiation as compared with early initiation of RRT.
訂閱:
文章 (Atom)