Topic: Pathophysiology of Renal Tubular Acidosis: Core Curriculum 2016 -- Hyperkalemic RTA (type 4)
| ||
整理
|
內容
=> most common: hypo-aldosteronism w/ hyperkalemia
=> pesistent hyperkalemia without obvious cause (eg, kidney failure, use of K supplements, or K-sparing diuretics)
| |
摘要
| ||
2016年5月31日 星期二
2016 AJKD--Pathophysiology of Renal Tubular Acidosis: Core Curriculum 2016 -- Hyperkalemic RTA (type 4)
2009 NDT--Systematic review of antimicrobials for the prevention of haemodialysis catheter-related infections
2009 NDT--Systematic review of antimicrobials for the prevention of haemodialysis catheter-related infections
Conclusion. The use of AMLs and exit-site antimicrobials
are useful measures in the reduction of CRIs, whereas antimicrobial impregnated catheters and peri-operative systemic antimicrobial administration have not been found to
be beneficial. Further head-to-head trials of various AMLs
and exit-site antimicrobials are needed to know about their
comparative clinical efficacy.
因此,abx lock therapy or exit site abx 是有效預防CRBSI;
但是術前後中後術prophylatic abx或是把catheter浸泡在abx中,似乎沒有benefit for prevention CRBSI
2011 IDSA guideline有提到,如果是dialysis catheter可以考慮使用topical abx,
不過倒是沒有說要用哪種topical abx
因此,abx lock therapy or exit site abx 是有效預防CRBSI;
但是術前後中後術prophylatic abx或是把catheter浸泡在abx中,似乎沒有benefit for prevention CRBSI
2011 IDSA guideline有提到,如果是dialysis catheter可以考慮使用topical abx,
不過倒是沒有說要用哪種topical abx
2016年5月30日 星期一
2004 AJKD--Dialysis catheter-related bacteremia: treatment and prophylaxis. vs. 2004 AJMS--Hemodialysis vascular catheter-related bacteremia.
Dialysis catheter-related bacteremia: treatment and prophylaxis.
More recent studies suggested that instillation of an antibiotic-anticoagulant lock into the catheter lumen, as an adjunct to systemic antibiotic therapy, can cure approximately two thirds of catheter-related bacteremias without requiring catheter replacement.用lock therapy for perm cath (suspected Perm cath related CRBSI) 只有三分之二的成功率,而不用換掉。其實成功率還是不夠高。
Hemodialysis vascular catheter-related bacteremia.
Bacteremia in patients with catheters results from luminal or extraluminal contamination and may be perpetuated by infected fibrin sheaths associated with the catheter. Bacteremic patients require antibiotic therapy and catheter removal. Guide wire catheter exchange is appropriate in stable patients, but catheter removal and later reinsertion of a new catheter is indicated for tunnel infection or frank sepsis.看來,要in-line change,並不建議在tunnelled catheter,而比較適合用在non-tunnelled catheter(?)。
當然,在IDSA 2011年的guideline也沒有絕對禁止in-line change這件事。
2012 QJM--Vascular access type and risk of mortality in a national prospective cohort of haemodialysis patients.
2012 QJM--Vascular access type and risk of mortality in a national prospective cohort of haemodialysis patients.
Conclusions: Compared with an arteriovenous fistula or graft, sustained use of tunnelled CVCs for vascular access is associated with higher risks of all-cause, cardiovascular and infection-related mortality.
因此,能用AVF or AVG就用;不行再考慮裝Tunnelled catheter
Conclusions: Compared with an arteriovenous fistula or graft, sustained use of tunnelled CVCs for vascular access is associated with higher risks of all-cause, cardiovascular and infection-related mortality.
因此,能用AVF or AVG就用;不行再考慮裝Tunnelled catheter
2016 AJKD--Pathophysiology of Renal Tubular Acidosis: Core Curriculum 2016 -- dRTA dx and Mx
Topic: Pathophysiology of Renal Tubular Acidosis: Core Curriculum 2016 -- dRTA dx and Mx
| |
整理
|
內容
=> decreased NH4 => NAE reduced + titratable acid excreetion + HCO3 wasting
=> serum HCO3 decreased + hyperchloremic metabolic acidosis
2. CD’s H secretion abnormality: 1) H-ATPase, cytosolic CA II, or kidney AE1 defect
=> failed to trapping of luminal NH3
3. Unique feature: 1. very low urinary citrate levels <= proximal tubule increased reabsorption of citrate in response to intracellular acidosis => less stone
4. hereditary dRTA vs. acquired dRTA => if mutations in CA II impaired HCO3 reabsorption in the proixmal tubule and collecting duct (mixed dRTA and pRTA (type III RTA) => affecting bone osteoclast resulting in osteopetrosis
5. Clinical picture:
<=> hyper-Cl metabolic acidosis <= diarrhea: UAG<0 + high UOG
6. Tx of dRTA: daily loss of HCO3: 1~2 mEq/kg/d => required 4~8mEq/kg/d to supply
7. Imcomplete dRTA: normal serum HCO3 while lacking the ability to acidify urien when challenged with an acid loading test
8. More severe hypokalemia in dRTA than pRTA
|
摘要
| |
2016年5月28日 星期六
Topic: Pathophysiology of Renal Tubular Acidosis: Core Curriculum 2016 pRTA Dx and Tx
Topic: Pathophysiology of Renal Tubular Acidosis: Core Curriculum 2016
pRTA Dx and Tx
| |
整理
|
內容
Acquired: tubular injury => light chain, amyloidosis, MM, autoimmune disorder, toxin, etc.
Tx w/ HCO3 (1~2 mEq/kg/d) 2~3 wks => recheck serum HCO3 => pRTA: serum HCO3 still significantly below normal + Alkaline urine pH
=> c.f. dRTA: nearly normal reference of serum HCO3
|
摘要
| |
2016年5月27日 星期五
Short term antibiotic strategy (episode control strategy) for infection control
Short term antibiotic strategy (episode control strategy) for infection control
2011 CID--Strategies for Reduction in Duration of Antibiotic Use in Hospitalized Patients
On the basis of published RCTs, shorter treatment durations seem just as likely as more prolonged, traditional regimens to cure most common bacterial infections.
2011 Critical Care--Duration of antibiotic therapy for bacteremia: a systematic review and meta-analysis
No significant differences in clinical cure, microbiologic cure and survival were detected among bacteremic patients receiving shorter versus longer duration antibiotic therapy. An adequately powered randomized trial of bacteremic patients is needed to confirm these findings.
• The optimal duration of treatment for bloodstream infections is understudied.
• Available data from bacteremic subgroups of prior randomized controlled trials suggest that shorter duration therapy (not more than 7 days) may be as effective as longer-duration therapy in achieving clinical cure, microbiologic cure, and survival among most patients with bloodstream infections.
• A large dedicated randomized trial of treatment duration for bacteremia is urgently needed.
2015 NEJM--Trial of Short-Course Antimicrobial Therapy for Intraabdominal Infection control
In patients with intraabdominal infections who had undergone an adequate source control procedure, the outcomes after fixed-duration antibiotic therapy (approximately 4 days) were similar to those after a longer course of antibiotics (approximately 8 days) that extended until after the resolution of physiological abnormalities
2016年5月22日 星期日
2016年5月10日 星期二
ACEi vs ARB in Scleroderma with renal crisis
雖然它們都跟RAS inhibition有關 ACEi 與ARB終究還是屬於不同的東西 Scleroderma with renal involvement (SSc),
short-acting ACEi 還是優先於ARB 的使用,
當ACEi 的額度用滿了,ARB還可以考慮作為add-on
( by Harrison, 19/e; Washington, 35/e; and Brenner, 10/e)
BUT,遇到了Scleroderma with vascular involvement的時候,
ARB卻比起ACEi 來得有效(effective)(by Harrison, 19/e) 結論就是說當遇到了systemic sclerosis with renal crisis時,
要記得給short-acting ACEi 雖然文獻不多,
Brenner仍然舉了二篇case report來說明ACEi is better than ARB in scleroderma with renal crisis. 2005 AJKD--Late Recurrence of Scleroderma Renal Crisis in a Renal Transplant Recipient Despite Angiotensin II Blockade
1997 Lancet--Failure of losartan to control blood pressure in scleroderma renal crisis
Metabolic alkalosis with/without Cl responsiveness
Metabolic alkalosis with/without Cl responsiveness
The Brenner and Rector's: The Kidney, 10/e

2016年5月9日 星期一
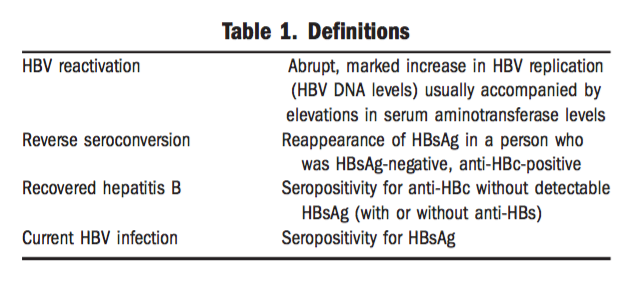
Overt and Occult HBV carriers and reverse seroconversion
Overt HBV carriers (HBsAg (+)):
- Active carriers: HBeAg(+) + HBV viral load
- Inactive carriers: HBeAg (-) or anti-HBe + HBV viral load
Occult HBV carriers (HBsAg (-)):
- anti-HBc(+) ± anti-HBs => potential occult carriers


2007 Digestive and Liver Disease--Prophylaxis and treatment of hepatitis B in immunocompromised patients
2015 Hepatology--Recent US Food and Drug Administration Warnings on Hepatitis B Reactivation With Immune-Suppressing and Anticancer Drugs- Just the Tip of the Iceberg?
RTA 比較
RTA 比較
RTA 1
|
RTA 2
|
RTA 4
| |
dysfunction site
|
distal
|
proximal
|
aldosterone
|
Renin/Aldosterone
|
low/low
| ||
HCO3 loss
(FeHCO3)
|
loss
(FeHCO3 >15%)
|
↓
| |
H gain
|
retention
|
↓
| |
serum K
|
low
|
low
|
high
|
AG mat. acidosis
|
non-AG
| ||
UAG
|
>0
|
<0 or >0
|
>0
|
Examples
|
Sjogren’s. RA, Li, Amp-B
|
MM, Fanconi’s
|
DMN, ACEi
|
例外
|
K高 => sickle cell, obstr. SLE, renal transplant
| ||
2016年5月8日 星期日

Measles
Measles
- 第二類法定傳染病
- 症狀:高燒、鼻炎、結膜炎、咳嗽 => 內頰側黏膜上有柯氏斑點(Koplik spots)
=> 耳後典型斑丘疹 => 擴散到臉面 => 軀幹和四肢
=> 鱗屑性脫皮+褐色沈著,有時會有secondary infection to bacteria or virus
=> complications:中耳炎、肺炎、腦炎
- measles virus ( 麻疹病毒)
- Reservoir:人為唯一之宿主及傳染窩(reservoir)
- 傳染方式:空氣、飛沫傳播、病人鼻腔/咽喉分泌物
- 潛伏期:7~18天,通常14天(自暴露到紅疹出現);
可傳染期:發疹前後4天
- 可以終身免疫
- 診斷:
- serum IgM or IgG titer > = 4倍上升;採檢時間為出疹後3~28天,第二次探血要隔2~4週(14天~28天)
- 尿液/咽喉檢體:real-time PCR and virus isolation ;採檢時間為出疹後7天內
- 2009年4月開始MMR第一劑改為出生滿12個月接種
- 通報:24小時內
- 通報定義:rash + fever (>=38C),+以下三者任一:
- 咳嗽、流鼻水,或結膜炎(三取一)
- 無麻診相關疫苗接種史
- 發病前三週內,曾有麻疹流行地區旅遊史
- 住院病人需呼吸道隔離(respiratory isolation),以避免院內感染
訂閱:
意見 (Atom)